Malaria is a severe disease caused by parasites of the genus Plasmodium, which is transmitted to humans by a bite of an infected female mosquito of the species Anopheles. Malaria remains the leading cause of mortality around the world, and early diagnosis and fast-acting treatment prevent unwanted outcomes. It is the most common disease in Africa and some countries of Asia, while in the developed world malaria occurs as imported from endemic areas. The sweet sagewort plant was used as early as the second century BC to treat malaria fever in China. Much later, quinine started being used as an antimalaria drug. A global battle against malaria started in 1955. The World Health Organization carries out a malaria control program on a global scale, focusing on local strengthening of primary health care, early diagnosis of the disease, timely treatment, and disease prevention. Globally, the burden of malaria is lower than ten years ago. However, in the last few years, there has been an increase in the number of malaria cases around the world. It is moving towards targets established by the WHO, but that progress has slowed down.
- Anopheles
- antimalarials
- malaria
- Plasmodium
1. Introduction
Introduction
Plasmodium
Plasmodium
Plasmodium
Plasmodium
P. malariae, P. falciparum, P. vivax, P. ovale
P. knowlesi
P. knowlesi
Plasmodium
Malus aer
Plasmodium
Anopheles
Plasmodium
Plasmodium
P. vivax
P. malariae
P. falciparum
14].
2. Discovery of Malaria
It is believed that the history of malaria outbreaks goes back to the beginnings of civilization. It is the most widespread disease due to which many people have lost lives and is even thought to have been the cause of major military defeats, as well as the disappearance of some nations []. The first descriptions of malaria are found in ancient Chinese medical records of 2700 BC, and 1200 years later in the Ebers Papyrus []. The military leader Alexander the Great died from malaria []. The evidence that this disease was present within all layers of society is in the fact that Christopher Columbus, Albrecht Dürer, Cesare Borgia, and George Washington all suffered from it [,]. Although the ancient people frequently faced malaria and its symptoms, the fever that would occur in patients was attributed to various supernatural forces and angry divinities. It is, thus, stated that the Assyrian-Babylonian deity Nergal was portrayed as a stylized two-winged insect, as was the Canaan Zebub (‘Beelzebub, in translation: the master of the fly’) []. In the 4th century BC, Hippocrates described this disease in a way that completely rejected its demonic origins and linked it with evaporation from swamps which, when inhaled, caused the disease. That interpretation was maintained until 1880 and Laveran’s discovery of the cause of the disease []. Laveran, a French military surgeon, first observed parasites in the blood of malaria patients, and for that discovery, he received the Nobel Prize in 1907 []. Cartwright and Biddis state that malaria is considered to be the most widespread African disease []. The causative agent of malaria is a small protozoon belonging to the group ofPlasmodium
species, and it consists of several subspecies [14].
].3. The Development of Diagnostic Tests for Proving Malaria through History
Malaria can last for three and up to five years, if left untreated, and depending on the cause, may recrudesce. InP. vivax
andovale
infections, the persistence of the merozoites in the blood or hypnozoites in hepatocytes can cause relapse months or years after the initial infection. Additionally, relapse of vivax malaria is common afterP. falciparum
infection in Southeast Asia. Relapse cases were observed inP. falciparum
infections, which can lead to a rapid high parasitemia with subsequent destruction of erythrocytes [,]. Children, pregnant women, immunocompromised and splenectomized patients are especially vulnerable to malaria infection, as well as healthy people without prior contact withPlasmodium
. A laboratory test for malaria should always confirm clinical findings. The proving of malaria is carried out by direct methods such as evidence of parasites or parts of parasites, and indirect methods that prove the antibodies to the causative agents () [,,].| Advantages | Disadvantages | |
|---|---|---|
| Direct methods | ||
| Microscopic analysis | Fast test, cheap | Required much experience as well as equipment |
| Rapid diagnostic tests | Quick and simple | Less sensitive and accurate, price |
| Molecular tests | Correct determination of type, highly sensitive and accurate | Price, long-term in a large number of cases |
| Indirect methods | ||
| Indirect immunofluorescence | Specific, sensitive | Long time to perform, subjective evaluation of results |
| ELISA | Correct determination of type, specific, sensitive | Long time to perform, price |
P. falciparum
orP. vivax
infections or both []. False-positive rates ofP. vivax
were typically small, between 5% and 15%. On the other hand, the false-positive rates ofP. falciparum
range from 3–32% [,]. Good RDTs might occasionally give false-negative results if the parasite density is low, or if variations in the production of parasite antigen reduce the ability of the RDT to detect the parasite. False negative results of the RDT test forP. falciparum
ranged between 1% and 11% [,,,]. The overall sensitivity of RDTs is 82% (range 81–99%), and specificity is 89% (range 88–99%) []. Polymerase chain reaction (PCR) is another method in the detection of malaria. This method is more sensitive and more specific than all conventional methods in the detection of malaria. It can detect below one parasite/μL. PCR test confirms the presence of parasitic nucleic acid [,]. PCR results are often not available fast enough to be useful in malaria diagnosis in endemic areas. However, this method is most helpful in identifyingPlasmodium
species after diagnosis by microscopy or RDT test in laboratories that might not have microscopic experts. Additionally, PCR is useful for the monitoring of patients receiving antimalaria treatment [,]. Indirect methods are used to demonstrate antibodies to malaria-causing agents. Such methods are used in testing people who have been or might be at risk of malaria, such as blood donors and pregnant women. The method is based on an indirect immunofluorescence assay (IFA) or an ELISA test. The IFA is specific and sensitive but not suitable for a large number of samples, and the results are subjective evaluations. For serological testing, ELISA tests are more commonly used [26].
]. Rapid and accurate diagnosis of malaria is an integral part of appropriate treatment for the affected person and the prevention of the further spread of the infection in the community.Rapid and accurate diagnosis of malaria is an integral part of appropriate treatment for the affected person and the prevention of the further spread of the infection in the community.
4. Malaria Treatment through History
Already in the 2nd century BC, a sweet sagewort plant named Qinghai (LatinArtemisia annua
) was used for the treatment of malaria in China []. Much later, in the 16th century, the Spanish invaders in Peru took over the cinchona medication against malaria obtained from the bark of the Cinchona tree (LatinCinchona succirubra
). From this plant in 1820 the French chemists, Pierre Joseph Pelletier, and Joseph Bienaimé Caventou isolated the active ingredient quinine, which had been used for many years in the chemoprophylaxis and treatment of malaria. In 1970, a group of Chinese scientists led by Dr. Youyou Tu isolated the active substance artemisinin from the plantArtemisia annua
, an antimalarial that has proved to be very useful in treating malaria. For that discovery, Youyou Tu received the Nobel Prize for Physiology and Medicine in 2015 [,,]. Most of the artemisinin-related drugs used today are prodrugs, which are activated by hydrolysis to the metabolite dihydroartemisinin. Artemisinin drugs exhibit its antimalarial activity by forming the radical via a peroxide linkage []. WHO recommends the use of artemisinin-based combination therapies (ACT) to ensure a high cure rate ofP. falciparum
malaria and reduce the spread of drug resistance. ACT therapies are used due to high resistance to chloroquine, sulfadoxine-pyrimethamine, and amodiaquine []. Due to the unique structure of artemisinins, there is much space for further research. Extensive efforts are devoted to clarification of drug targets and mechanisms of action, the improvement of pharmacokinetic properties, and identifying a new generation of artemisinins against resistantPlasmodium
strains []. The German chemist Othmer Zeidler synthesized dichlorodiphenyltrichloroethane (DDT) in 1874 during his Ph.D. At that time, no uses of DDT was found, and it just became a useless chemical []. The insecticide property of DDT was discovered in 1939 by Paul Müller in Switzerland. DDT began to be used to control malaria at the end of the Second World War []. During the Second World War, the success of DDT quickly led to the introduction of other chlorinated hydrocarbons which were used in large amounts for the control of diseases transmitted by mosquito []. From the late Middle Ages until 1940, when DDT began to be applied, two-thirds of the world’s population had been exposed to malaria, a fact that represented a severe health, demographic, and economic problem [,,,,]. DDT is an organochlorine pesticide which was applied in liquid and powder form against the insects. During the Second World War, people were sprayed with DDT. After the war, DDT became a powerful way of fighting malaria by attacking the vector []. Five Nobel Prizes associated with malaria were awarded: Youyou Tu in 2015. Ronald Ross received the Nobel Prize in 1902 for the discovery and significance of mosquitoes in the biology of the causative agents in malaria. In 1907, the Nobel was awarded to the already-mentioned Charles Louis Alphonse Laveran for the discovery of the causative agent. Julius Wagner-Jauregg received it in 1927 for the induction of malaria as a pyrotherapy procedure in the treatment of paralytic dementia. In 1947 Paul Müller received it for the synthetic pesticide formula dichlorodiphenyltrichloroethane. Attempts to produce an effective antimalarial vaccine and its clinical trials are underway. Over the past several decades’ numerous efforts have been made to develop effective and affordable preventive antimalaria vaccines. Numerous clinical trials are completed in the past few years. Nowadays are ongoing clinical trials for the development of next-generation malaria vaccines. The main issue isP. vivax
vaccine, whose research requires further investigations to identify novel vaccine candidates [,,]. Despite decades of research in vaccine development, an effective antimalaria vaccine has not yet been developed (i.e., with efficacy higher than 50%) [,,]. The European Union Clinical Trials Register currently displays 48 clinical trials with a EudraCT protocol for malaria, of which 13 are still ongoing clinical trials []. The malaria parasite is a complex organism with a complex life cycle which can avoid the immune system, making it very difficult to create a vaccine. During the different stages of thePlasmodium
life cycle, it undergoes morphological changes and exhibits antigenic variations.Plasmodium
proteins are highly polymorphic, and its functions are redundant. Also, the development of malaria disease depends on thePlasmodium
species. That way, a combination of different adjuvants type into antigen-specific formulations would achieve a higher efficacy [,]. Drugs that underwent clinical trials proved to be mostly ineffective [,,]. However, many scientists around the world are working on the development of an effective vaccine [,,]. Since other methods of suppressing malaria, including medication, insecticides, and bed nets treated with pesticides, have failed to eradicate the disease, and the search for a vaccine is considered to be one of the most important research projects in public health by World Health Organization (WHO). The best way to fight malaria is to prevent insect bites. Malaria therapy is administered using antimalarial drugs that have evolved from quinine. According to its primary effect, malarial vaccines are divided into pre-erythrocytic (sporozoite and liver-stage), blood-stage, and transmission-blocking vaccines [,]. Most medications used in the treatment are active against parasitic forms in the blood (the type that causes disease) () []. The two crucial antimalarial medications currently used are derived from plants whose medical importance has been known for centuries: artemisinin from the plant Qinghao (Artemisia annua
L, China, 4th century) and quinine fromCinchona
(South America, 17th century). Side-by-side with artemisinin, quinine is one of the most effective antimalarial drugs available today [,,]. Doxycycline is indicated for malaria chemoprophylaxis for travel in endemic areas. It is also used in combination with the quinine or artesunate for malaria treatment when ACT is unavailable or when the treatment of severe malaria with artesunate fails. The disadvantage of doxycycline is that children and pregnant women cannot use it []. Due to the global resistance ofP. falciparum
to chloroquine, ACTs are recommended for the treatment of malaria, except in the first trimester of pregnancy. ACTs consist of a combination of an artemisinin derivative that fast decreases parasitemia and a partner drug that eliminates remaining parasites over a more extended period. The most common ACTs in use are artemether-lumefantrine, artesunate-amodiaquine, dihydroartemisinin-piperaquine, artesunate-mefloquine, and artesunate with sulfadoxine-pyrimethamine. The ACTs were very efficient against allP. falciparum
until recently when numbers of treatment failures raised in parts of Southeast Asia. Atovaquone-proguanil is an option non-artemisinin-based treatment that is helpful for individual cases which have failed therapy with usual ACTs. Although, it is not approved for comprehensive implementation in endemic countries because of the ability for the rapid development of atovaquone resistance. Quinine remains efficient, although it needs a long course of treatment, is poorly tolerated, especially by children, and must be combined with another drug, such as doxycycline or clindamycin. Uncomplicated vivax, malariae, and ovale malaria are handled with chloroquine except in case of chloroquine-resistantP. vivax
when an ACT is used [,,,,].| Medication Name | Year of Discovery/Synthesis | Origin | Usage | Mechanism of Action | Side Effects | Advantages/Disadvantages | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Quinine | 1600 | Cinchona | tree, South America | Resistance to chloroquine, prophylaxis, and treatment of malaria | Inhibition of DNA and RNA synthesis | Headache, abortion, or congenital malformations if taken during pregnancy | Toxic, less effective than other medication | |||||||
| Chloroquine | 1934 | Synthesized by German scientist Hans Andersag | A most powerful remedy for the prophylaxis and treatment of malaria | Inhibition of DNA and RNA synthesis | Gastrointestinal disturbances, headache, skin irritation | Developed resistance of most strains | of P. falciparum | to the medication | ||||||
| Primaquine | 1953 | The 8-aminoquinoline derivative | Infections with | P. vivax | and | P. ovale | , prophylaxis and treatment of malaria | Interferes in transport chain of electrons and destroys parasite mitochondria | Anorexia, nausea, anemia, headaches, contraindicated in pregnancy and children under 4 years of age | Prevent relapse in | P. vivax | and | P. ovale | infection |
| Doxycycline | 1960 | Pfizer Inc. New York | Prophylaxis in areas with chloroquine resistance and against mefloquine-resistant | P. falciparum | Inhibition of protein synthesis by binding to 30S ribosomal subunit | Gastrointestinal disorders, nausea, vomiting, photosensitivity | Effective and cheap, use for treatment and prophylaxis in all malarious areas | |||||||
| Mefloquine | 1971 | USA army and WHO | Multiresistant | P. falciparum | strains, prophylaxis, and treatment of malaria | Damage to parasite membrane | Gastrointestinal disorders, CNS disorder, contraindicated in pregnancy and patients with epilepsy | Partial resistance, brain damage | ||||||
| Proguanil (chloroguanide) | 1953 | Biguanide derivate | Prophylaxis in infections with | P. falciparum | Inhibition of DNA synthesis | Digestive problems only in large doses | The least toxic antimalarial drug | |||||||
| Pyrimethamine | 1953 | Pyrimidine derivatives | For tissue parasites, prophylaxis, and treatment of malaria | Folic acid antagonist | Gastrointestinal disorders, neuropathy, in high doses also megaloblastic anemia | The rapid development of resistance | ||||||||
| Atovaquone/proguanil | 2000 | Ubiquinone analog | For the prophylaxis and treatment of malaria | Inhibition of cytochrome bc1 in | Plasmodium | Nausea, vomiting, diarrhea, headache, dizziness, anxiety, difficulty falling asleep, rash, fever | Most commonly used, fewer side effects and more expensive than mefloquine, | P. falciparum resistance |
4. Malaria in Europe
Malaria in Europe
Anopheles
4.1 Malaria in Croatia
Malaria in Croatia
Gambusia holbrooki
73]. In 1930 legislation was passed to enforce village sanitation, which included the construction of water infrastructure and safe wells, contributing to the prevention of malaria. Regular mosquito fogging with arsenic green (copper acetoarsenite) was introduced, and larvicidal disinfection of stagnant water was carried out.
79].
81].
Plasmodium
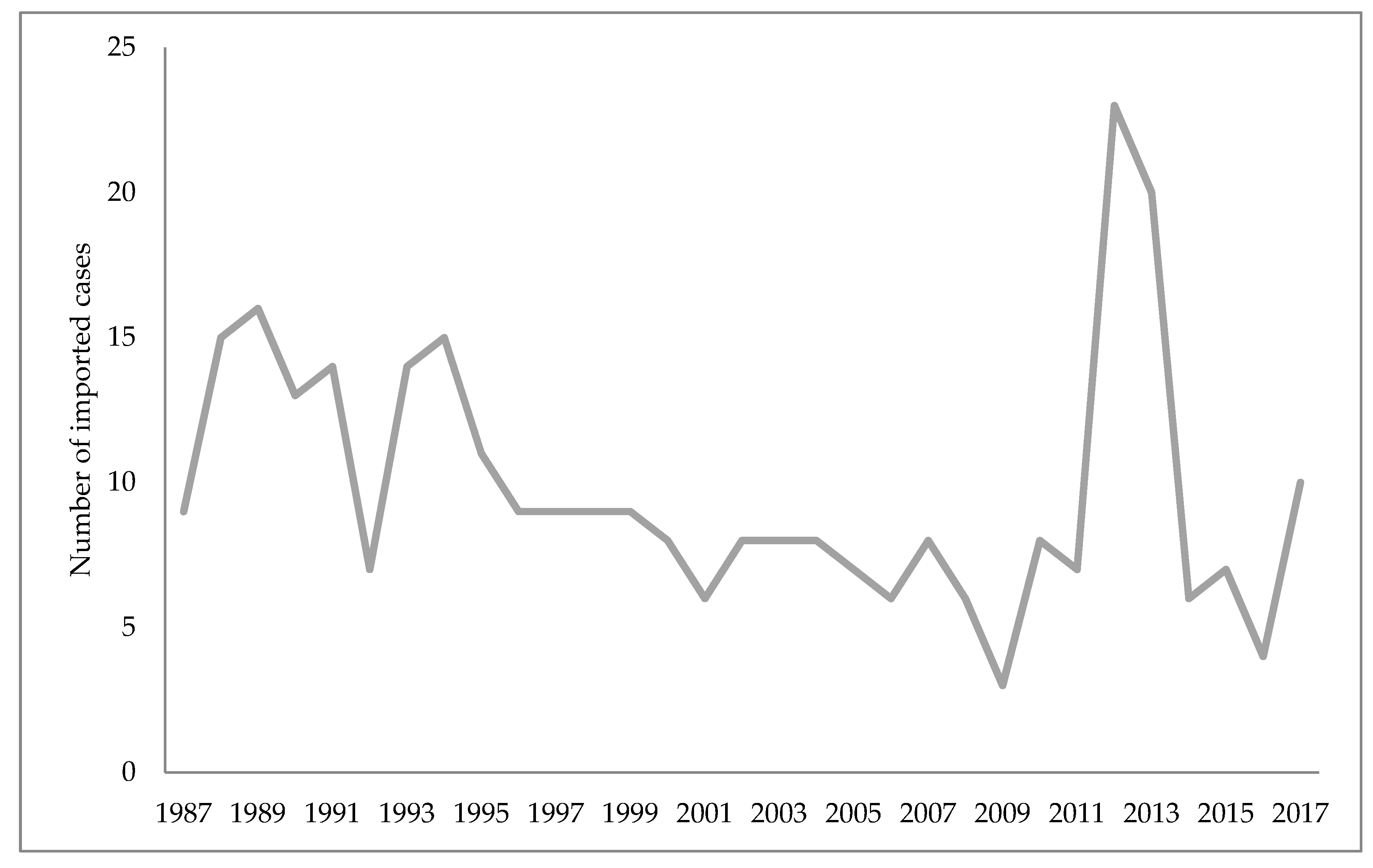
Anopheles, which means that the conditions of transmission of the imported malaria from the endemic areas still exist. The risk of malaria recrudesce is determined by the presence of the vector, but also by the number of infected people in the area. Due to climate change, it is necessary to monitor the vectors and people at risk of malaria. Naturally- and artificially-created catastrophes, such as wars and mass people migration from endemic areas, could favor recrudescing of malaria. Once achieved, eradication would be maintained if the vector capacities are low and prevention measures are implemented. The increased number of malaria cases worldwide, the recrudesce of indigenous malaria cases in the countries where the disease has been eradicated, the existence of mosquitoes that transmit malaria and the number of imported malaria cases in Croatia are alarming facts. Health surveillance, including obligatory and appropriate prophylaxis for travelers to endemic areas, remains a necessary public health care measure pointed at managing malaria in Croatia.
5. Malaria Trends in the World
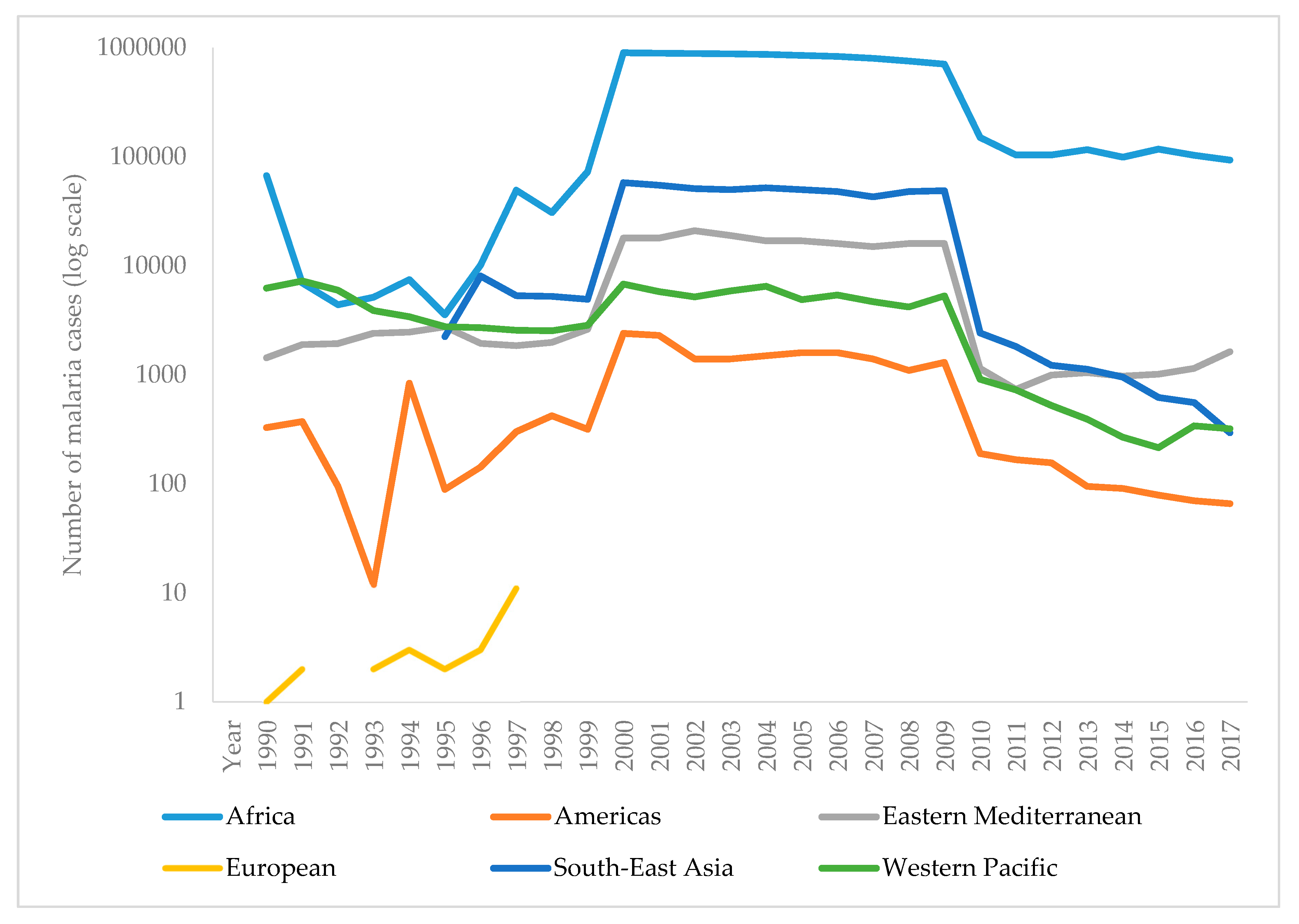
The WHO report on malaria in 2017 shows that it is difficult to achieve two crucial goals of a Global Technical Strategy for Malaria. These are a reduction in mortality and morbidity by at least 40% by 2020. Since 2010, there has been a significant reduction in the burden of malaria, but analysis suggests a slowdown and even an increase in the number of cases between 2015 and 2017. Thus, the number of malaria cases in 2017 has risen to 219 million, compared to 214 million cases in 2015 and 239 million cases in 2010. presents the reported number of malaria cases per WHO region from 1990–2017 [,]. The most critical step in the global eradication of malaria is to reduce the number of cases in countries with the highest burden (many in Africa). The number of deaths from disease is declining, thus, in 2017 there were 435,000 deaths from malaria globally, compared with 451,000 in 2016, and 607,000 deaths in 2010. presents the number of malaria deaths from 1990-2017 [,]. Despite the delay in global progress, there are countries with decreasing malaria cases during 2017. Thus, India in 2017, compared with 2016, recorded a 24% decline of malaria cases. The number of countries reporting less than 10,000 malaria cases is growing, from 37 countries in 2010, to 44 in 2016, and to 46 in 2017. Furthermore, the number of countries with fewer than 100 indigenous malaria cases growing from 15 in 2010, to 26 countries in 2017 [].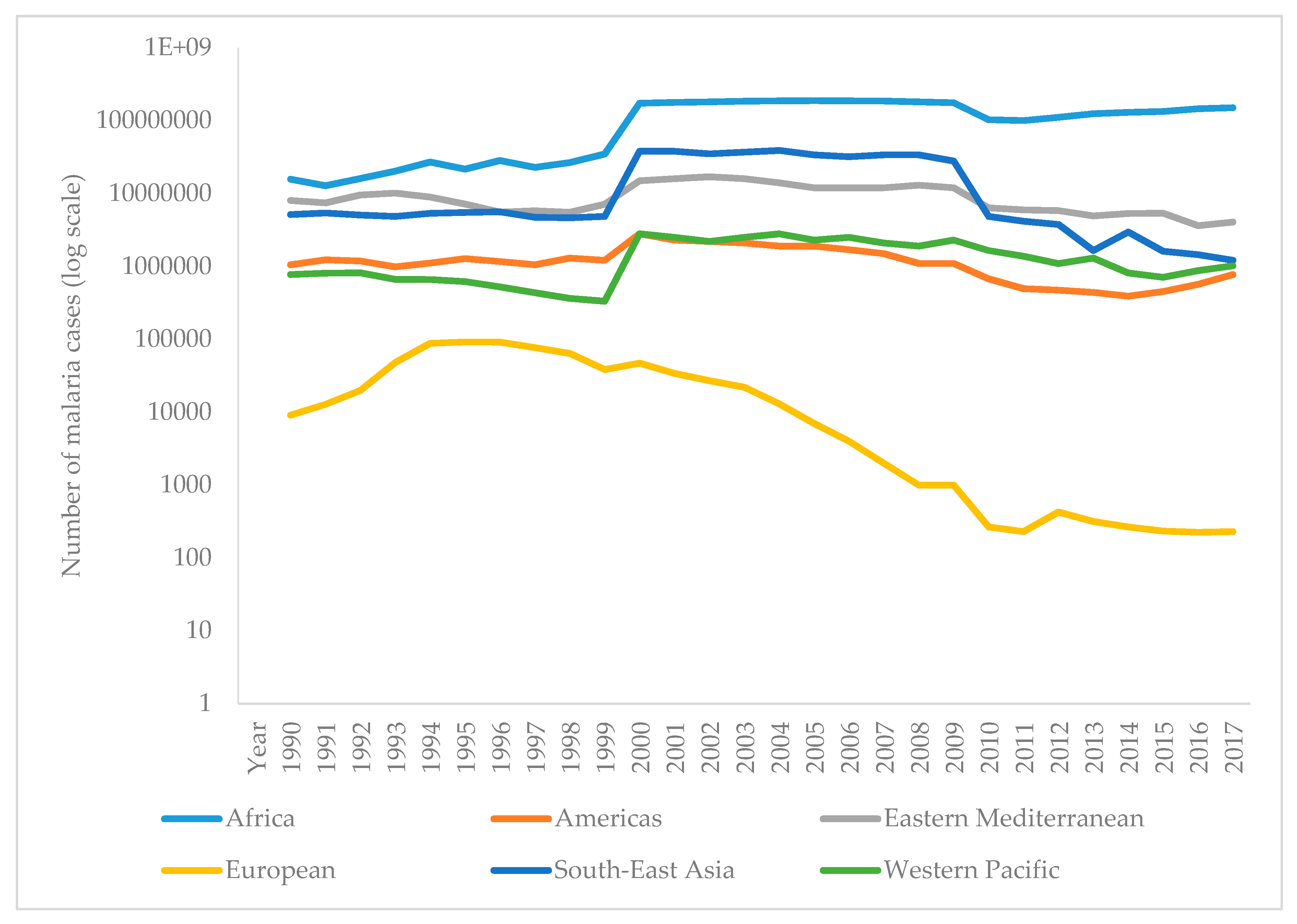
vivax
knowlesi
7]
References
- World Health Organization. World Malaria Report 2018; WHO: Geneva, Switzerland,
- White, N.J.N.; Pukrittayakamee, S.; Hien, T.T.T.; Faiz, M.A.; Mokuolu, O.A.O.; Dondorp, A.A.M. Malaria. Lancet 2014, 383, 723–735, doi:10.1016/S0140-6736(13)60024-0.
- Pan American Health Organization; World Health Organization. Epidemiological Alert, Increase of Malaria in the Americas; PAHO: Washington, DC, USA, 2018.
- Dhiman, S. Are malaria elimination efforts on right track? An analysis of gains achieved and challenges ahead. Dis. Poverty 2019, 8, 14, doi:10.1186/s40249-019-0524-x.
- Walker, N.; Nadjm, B.; Whitty, C. Malaria. Medicine 2017, 42, 52–58, doi:10.1016/j.mpmed.2013.11.011.
- Antinori, S.; Galimberti, L.; Milazzo, L.; Corbellino, M. Biology of human malaria plasmodia including Plasmodium knowlesi. J. Hematol. Infect. Dis. 2012, 4, e2012013, doi:10.4084/MJHID.2012.013.
- Ashley, E.A.; Pyae Phyo, A.; Woodrow, C.J. Malaria. Lancet 2018, 391, 1608–1621, doi:10.1016/S0140-6736(18)30324-6.
- Singh, B.; Daneshvar, C. Human Infections and Detection of Plasmodium knowlesi. Microbiol. Rev. 2013, 26, 165–184, doi:10.1128/CMR.00079-12.
- Vuk, I.; Rajic, Z.; Zorc, B. Malaria and antimalarial drugs. Farm Glas 2008, 64, 51–60.
- Soulard, V.; Bosson-Vanga, H.; Lorthiois, A.; Roucher, C.; Franetich, J.-F.; Zanghi, G.; Bordessoulles, M.; Tefit, M.; Thellier, M.; Morosan, S.; et al. Plasmodium falciparum full life cycle and Plasmodium ovale liver stages in humanized mice. Commun. 2015, 6, 7690, doi:10.1038/ncomms8690.
- Josling, G.A.; Llinás, M. Sexual development in Plasmodium parasites: Knowing when it’s time to commit. Rev. Genet. 2015, 13, 573–587, doi:10.1038/nrmicro3519.
- Blut, A. Untergruppe “Bewertung Blutassoziierter Krankheitserreger.” Transfus. Med. Hemother. 2009, 36, 48–60, doi:10.1159/000197327.
- Cowman, A.; Healer, J.; Marapana, D.; Marsh, K. Malaria, Biology and Disease. Cell 2016, 167, 610–624, doi:10.1016/j.cell.2016.07.055.
- Cartwright, F.; Biddis, M. Disease and History; Naklada Ljevak: Zagreb, Croatia, 2006.
- Lehrer, S. Vitezi Medicine; Prosveta: Beograd, Serbia, 1981.
- Moss, W.; Shah, S.; Morrow, R. The History of Malaria and its Control. Encycl. Public Health 2008, 389–398, doi:10.1016/B978-012373960-5.00374-9.
- Dugacki, V. Dr. Rudolf Battara operation in Nin in 1902, the first systematic battle attempt against malaria in Croatia. Jaderina 2005, 35, 33–40.
- Jovic, S. Istorija Medicine i Zdravstvene Kulture na tlu Dansnje Vojvodine 1718–1849 II; dio. Matica srpska, Srpska akademija nauka i umetnosti: Novi Sad, Serbia, 1998.
- Tan, S.Y.; Ahana, A. Charles Laveran (1845–1922), Nobel laureate pioneer of malaria. Med. J. 2009, 50, 657–658.
- Saifi, M.A.; Wajihullah, Siddiqui, M.I.; Al-Khalifa, M.S.; Malaria: Patterns of relapse and resistance. King Saud Univ. Sci. 2010, 22, 31–36, doi:10.1016/J.JKSUS.2009.12.005.
- Chu, C.S.; White, N.J. Management of relapsing Plasmodium vivax malaria. Expert Rev. Anti-Infect. Ther. 2016, 14, 885, doi:10.1080/14787210.2016.1220304.
- Murphy, S.C.; Shott, J.P.; Parikh, S.; Etter, P.; Prescott, W.R.; Stewart, V.A. Malaria diagnostics in clinical trials. J. Trop. Med. Hyg. 2013, 89, 824–839, doi:10.4269/ajtmh.12-0675.
- Tangpukdee, N.; Duangdee, C.; Wilairatana, P.; Krudsood, S. Malaria diagnosis, a brief review. Korean J. Parasitol. 2009, 47, 93–102, doi:10.3347/kjp.2009.47.2.93.
- Trampuz, A.; Jereb, M.; Muzlovic, I.; Prabhu, R.M. Clinical review, Severe malaria. Care 2003, 7, 315–323, doi:10.1186/cc2183.
- She, R.C.; Rawlins, M.L.; Mohl, R.; Perkins, S.L.; Hill, H.R.; Litwin, C.M. Comparison of Immunofluorescence Antibody Testing and Two Enzyme Immunoassays in the Serologic Diagnosis of Malaria. Travel Med. 2007, 14, 105–111, doi:10.1111/j.1708-8305.2006.00087.x.
- Oh, J.S.; Kim, J.S.; Lee, C.H.; Nam, D.H.; Kim, S.H.; Park, D.W.; Lee, C.K.; Lim, C.S.; Park, G.H. Evaluation of a malaria antibody enzyme immunoassay for use in blood screening. Inst. Oswaldo Cruz 2008, 103, 75–78, doi:10.1590/S0074-02762008005000008.
- Kakkilaya, B. Rapid Diagnosis of Malaria. Med. 2003, 34, 602–608, doi:10.1309/J4ANKCCJ147JB2FR.
- Abba, K.; Kirkham, A.J.; Olliaro, P.L.; Deeks, J.J.; Donegan, S.; Garner, P.; Takwoingi, Y. Rapid diagnostic tests for diagnosing uncomplicated non-falciparum or Plasmodium vivax malaria in endemic countries. Cochrane Database Syst. Rev. 2014, 12, doi:10.1002/14651858.CD011431.
- World Health Organization. Guidelines for the Treatment of Malaria, 3rd ed.; WHO: Geneva, Switzerland, 2015.
- World Health Organization. Malaria Rapid Diagnostic Test Performance, Results of WHO Product Testing of Malaria RDTs, Round 8 (2016–2018); WHO: Geneva, Switzerland, 2018.
- Ranadive, N.; Kunene, S.; Darteh, S.; Ntshalintshali, N.; Nhlabathi, N.; Dlamini, N.; Chitundu, S.; Saini, M.; Murphy, M.; Soble, A. Limitations of Rapid Diagnostic Testing in Patients with Suspected Malaria, A Diagnostic Accuracy Evaluation from Swaziland, a Low-Endemicity Country Aiming for Malaria Elimination. Infect. Dis. 2017, 64, 1221, doi:10.1093/CID/CIX131.
- Berhane, A.; Russom, M.; Bahta, I.; Hagos, F.; Ghirmai, M.; Uqubay, S. Rapid diagnostic tests failing to detect Plasmodium falciparum infections in Eritrea, an investigation of reported false negative RDT results. J. 2017, 16, 105, doi:10.1186/s12936-017-1752-9.
- Kozycki, C.T.; Umulisa, N.; Rulisa, S.; Mwikarago, E.I.; Musabyimana, J.P.; Habimana, J.P.; Karema, C.; Krogstad, D.J. False-negative malaria rapid diagnostic tests in Rwanda: Impact of Plasmodium falciparum isolates lacking hrp2 and declining malaria transmission. J. 2017, 16, 123, doi:10.1186/s12936-017-1768-1.
- World Health Organization. False-negative RDT results and implications of new reports of P. falciparum histidine-rich protein 2/3 gene deletions. WHO 2017, doi:10.1186/1475-2875-10-166.
- Murray, C.K.; Gasser, R.A.; Magill, A.J.; Miller, R.S. Update on Rapid Diagnostic Testing for Malaria. Microbiol. Rev. 2008, 21, 97–110, doi:10.1128/CMR.00035-07.
- Mathison, B.A.; Pritt, B.S. Update on Malaria Diagnostics and Test Utilization. Clin. Microbiol. 2017, 55, 2009–2017, doi:10.1128/JCM.02562-16.
- Rougemont, M.; Van Saanen, M.; Sahli, R.; Hinrikson, H.P.; Bille, J.; Jaton, K. Detection of Four Plasmodium Species in Blood from Humans by 18S rRNA Gene Subunit-Based and Species-Specific Real-Time PCR Assays. Clin. Microbiol. 2004, 42, 5636–5643, doi:10.1128/JCM.42.12.5636-5643.2004.
- Hsu, E. The history of qing hao in the Chinese materia medica. R. Soc. Trop. Med. Hyg. 2006, 100, 505–508, doi:10.1016/j.trstmh.2005.09.020.
- Achan, J.; O Talisuna, A.; Erhart, A.; Yeka, A.; Tibenderana, J.K.; Baliraine, F.N.; Rosenthal, P.J.; D’Alessandro, U. Quinine, an old anti-malarial drug in a modern world: Role in the treatment of malaria. J. 2011, 10, 144.
- Meshnick, S.R.; Dobson, M.J. The History of Antimalarial Drugs. In Antimalarial Chemotherapy, Mechanisms of Action, Resistance, and New Directions in Drug Discovery; Rosenthal, P., Ed.; Humana Press: Totowa NJ, USA, 2001; p. 396.
- World Health Organization. Antimalarial Drug Combination Therapy. Report of a WHO Technical Consultation; WHO: Geneva, Switzerland, 2001.
- Guo, Z. Artemisinin anti-malarial drugs in China. Acta Pharm. Sin. B 2016, 6, 115–124, doi:10.1016/j.apsb.2016.01.008.
- Ray, D. Organochlorine and Pyrethroid Insecticides. Toxicol. 2010, 13, 445–457, doi:10.1016/B978-0-08-046884-6.01327-0.
- Flannery, E.L.; Chatterjee, A.K.; Winzeler, E.A. Antimalarial drug discovery—Approaches and progress towards new medicines. Rev. Microbiol. 2013, 11, 849–862, doi:10.1038/nrmicro3138.
- Zhao, X.; Smith, D.L.; Tatem, A.J. Exploring the spatiotemporal drivers of malaria elimination in Europe. J. 2016, 15, 122, doi:10.1186/s12936-016-1175-z.
- Karunamoorthi, K. Malaria vaccine, a future hope to curtail the global malaria burden. J. Prev. Med. 2014, 5, 529–538.
- Moreno, A.; Joyner, C. Malaria vaccine clinical trials, what’s on the horizon. Opin. Immunol. 2015, 35, 98–106, doi:10.1016/j.coi.2015.06.008.
- Coelho, C.H.; Doritchamou, J.Y.A.; Zaidi, I.; Duffy, P.E. Advances in malaria vaccine development, report from the 2017 malaria vaccine symposium. NPJ Vaccines 2017, 2, 34, doi:10.1038/s41541-017-0035-3.
- Mahmoudi, S.; Keshavarz, H. Efficacy of phase 3 trial of RTS, S/AS01 malaria vaccine, The need for an alternative development plan. Vaccines Immunother. 2017, 13, 2098–2101, doi:10.1080/21645515.2017.1295906.
- Rénia, L.; Goh, Y.S.; Peng,. K, Mauduit, M.; Snounou, G. Assessing Malaria Vaccine Efficacy. In Towards Malaria Elimination: A Leap Forw; Manguin, S., Dev, V., Eds.; IntechOpen: London, UK, 2018; pp. 339–362, doi:10.5772/intechopen.77044.
- Draper, S.J.; Sack, B.K.; King, C.R.; Nielsen, C.M.; Rayner, J.C.; Higgins, M.K.; et al. Malaria Vaccines, Recent Advances and New Horizons. Cell Host Microbe 2018, 24, 43–56, doi:10.1016/j.chom.2018.06.008.
- Clinical Trials Register—Clinical Trials for Malaria 2019. Available online: https://www.clinicaltrialsregister.eu/ctr-search/search?query=Malaria (accessed on 30 April 2019).
- Crompton, P.D.; Pierce, S.K.; Miller, L.H. Advances and challenges in malaria vaccine development. Clin. Investig. 2010, 120, 4168–4178, doi:10.1172/JCI44423.
- Arama, C.; Troye-Blomberg, M. The path of malaria vaccine development, challenges and perspectives. Intern. Med. 2014, 275, 456–466, doi:10.1111/joim.12223.
- Kisalu, N.K.; Idris, A.H.; Weidle, C.; Flores-Garcia, Y.; Flynn, B.J.; Sack, B.K.; Murphy, S.; Schön, A.; Freire, E.; Francica, J.R.; et al. A human monoclonal antibody prevents malaria infection by targeting a new site of vulnerability on the parasite. Med. 2018, 24, 408–416, doi:10.1038/nm.4512.
- Claudia, F. Malaria vaccine–is it still required? Are vaccine alternatives enough to achieve malaria control? Asian Pac. J. Trop. Biomed. 2014, 4, S541–S544, doi:10.12980/APJTB.4.2014APJTB-2014-0181.
- Greenwood, B.; Targett, G. Malaria vaccines and the new malaria agenda. Microbiol. Infect. 2011, 17, 1600–1607, doi:10.1111/j.1469-0691.2011.03612.x.
- Hoffman, S.L.; Vekemans, J.; Richie, T.; Duffy, P. The March Toward Malaria Vaccines. J. Prev. Med. 2015, 49, S319–S333, doi:10.1016/j.amepre.2015.09.011.
- Shingadia, D. Treating malaria in the UK. Child Health 2014, 24, 232–235, doi:10.1016/j.paed.2013.10.003.
- Kremsner, P.G.; Krishna, S. Antimalarial combinations. Lancet 2004, 364, 285–294, doi:10.1016/S0140-6736(04)16680-4.
- Price, R.N.; Douglas NM. Artemisinin combination therapy for malaria, beyond good efficacy. Infect. Dis. 2009, 49, 1638–1640, doi:10.1086/647947.
- Nabudere, H.; Upunda, G.L.; Juma, M. Policy brief on improving access to artemisinin-based combination therapies for malaria in the East African community. J. Technol. Assess Health Care 2010, 26, 255–259, doi:10.1017/S026646231000019X.
- Sallares, R. Malaria and Rome: A History of Malaria in Ancient Italy; Oxford University Press: Oxford, UK, 2002; doi:10.1093/acprof,oso/9780199248506.001.0001.
- Micallef, M.J. The Roman fever, observations on the understanding of malaria in the ancient Roman world. J. Aust. 2016, 205, 501–503, doi:10.5694/mja16.00206.
- Jugoslavenski Leksikografski Zavod. Medical Encycolpedia; Jugoslavenski Leksikografski Zavod: Zagreb, Yugoslavia, 1969; p. 374.
- Trausmiller, O. Malarija i civilizacija. Priroda 1936, 3, 76–83.
- Odolin, S.; Gautret, P.; Parola, P. Epidemiology of imported malaria in the mediterranean region. J. Hematol. Infect. Dis. 2012, 4, e2012031.
- World Health Organization. Fact Sheet—History of Malaria Elimination in the European Region; WHO: Geneva, Switzerland, 2016.
- Mlinaric, D. Eco-historical area of the istrian borderland as a framework of the development of endemic diseases. Istar. Arh. 2010, 17, 155–177.
- Radosevic, M. Health conditions in the municipality of Medulin through history. In Municipality of Medulin Monograph; Bader, A., Ed.; Opcina Medulin: Medulin, Croatia, 2013; pp. 314–325.
- Rudetic, I. Malaria. In Istarska Enciklopedija; Bertosa, M., Matijasic, R., Eds.; Leksikografski Zavod Miroslav Krleza: Zagreb, Croatia, 2005; p. 544.
- Bakic, J. Seven centuries of the prevention of spreading of the infectious diseases into Croatia—Overview of the 60th anniversary of establishment of modern pest control in Croatia. Cas. Zavod Javno Zdr. 2011, 7, 1–17.
- Bakic, J. Trust worthy facts on first medically-entomological laboratory and introduction of Gambusia holbrooki into Croatia. Cas. Zavod Javno Zdr. 2006, 2, 20–25.
- Nezic, E. Ribica gambuzija u borbi protiv malarije. J. Fish. 1938, 1, 62–66.
- Mulic, R.; Aljinovic, L.; Gizdic, Z.; Petri, N.M. Malaria in Republic of Croatia, past, present and future. Vjesn. 2000, 122, 51–55.
- Fortis, A. Put Po Dalmaciji; Globus: Zagreb, Croatia, 1984.
- Wokaunn, M.; Juric, I.; Vrbica, Z. Between stigma and dawn of medicine, the last leprosarium in Croatia. Med. J. 2006, 47, 759–766.
- Tomasic, P. Malarija i blagostanje čovjeka. Priroda 1947, 4, 126–130.
- Skenderovic, R. Health Reforms Introduced by Maria Theresa in Provincial Slavonia and Generale Normativum Sanitatis of 1770. Slavon. 2005, 5, 115–143.
- Von Taube, F.W. Slavonija i Srijem 1777./1778; Drzavni Arhiv u Osijeku: Osijek, Croatia, 2012.
- Holzer, A. Asaniranje domacih predjela malarije. Liecnicki Viest. 1877, 4, 56–59.
- Majcen, V. The film funds of the school of national health (Andrija Stampar) at the Croatian film-library within the Croatian archive. Vjesn. 1987, 30, 71–88.
- Miletic-Medved, M.; Bozikov, J.; Uzarević, Z. Branko Cvjetanovic i Branimir Richter—Suradnici Andrije Stampara. Zavoda Za Znan. Umjetnicki Rad Osijeku 2012, 28, 103–113.
- Piperaki, E.T.; Daikos, G.L. Malaria in Europe, emerging threat or minor nuisance? Microbiol. Infect. 2016, 22, 487–493, doi:10.1016/J.CMI.2016.04.023.
- Mulic, R. Malaria in Croatia, from eradication until today. J. 2012, 11, P135, doi:10.1186/1475-2875-11-S1-P135.
- Peric, D. Skrobonja, I.; Skrobonja, A.; Peric, D.; Skrobonja, I.; Skrobonja, A. Malaria in Croatia in the period between 1987 to 2006. Vjesn. 2009, 131, 192–195.
- Stevanovic, R.; Capak, K.; Brkic, K. Croatian Health Statistics Yearbook 2017; Croatian Institute of Public Health: Zagreb, Croatia, 2018.
- Talapko, J. Optimizacija metoda za uništavanje komaraca, ali i zaštite okoline. Vjesn. 1986, 2, 353–356.
- Tucak, A.; Dimitrijevic, M.; Gucunski, D.; Konstantinovic, B.; Miljus, B.; Grgic, Z.; Balog, Z.; Paulus, R.; Talapko, J. Multicentricni Program Istraživanja Ekologije Komaraca na Podrucju Sjeveroistocne Slavonije; Sveuciliste u Osijeku, Znanstvena Jedinica za Klinicko-Medicinska Istraživanja Opce bolnice Osijek: Osijek, Croatia, 1985.
- World Health Organization. World Malaria Report 2010; WHO: Geneva, Croatia, 2010.
- Patouillard, E.; Griffin, J.; Bhatt, S.; Ghani, A.; Cibulskis, R. Global investment targets for malaria control and elimination between 2016 and 2030. BMJ Glob. Health 2017, 2, e000176, doi:10.1136/bmjgh-2016-000176.
- World Health Organization. Global Report on Insecticide Resistance in Malaria Vectors, 2010–2016; WHO: Geneva, Croatia, 2018.
- Alonso, P.; Noor, A,M. The global fight against malaria is at crossroads. Lancet 2017, 390, 2532–2534, doi:10.1016/S0140-6736(17)33080-5.